Root Cause analysis using a combination of Fault Tree Analysis and 5 Whys
Uncovering the root causes of more complex problems
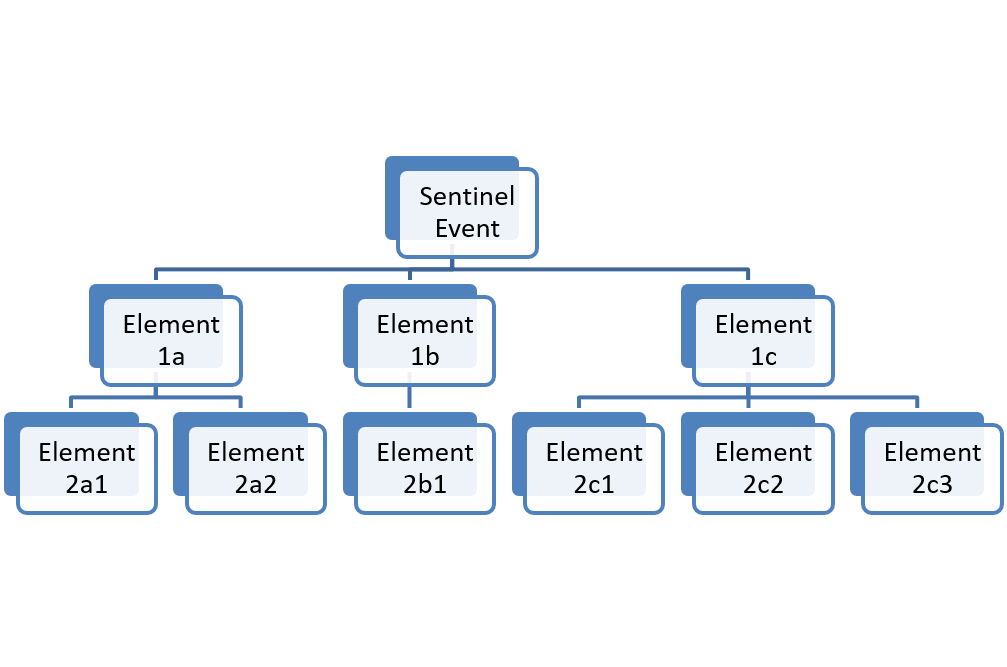
When you find a problem, this is called the sentinel event on the fault tree diagram, and it is listed at the top (Figure 1).
From there, ask why or how something went wrong to lead to that particular problem (failure or defect).
Then, you list in a row below the sentinel event the issues that have occurred to lead to the error.
This first row is typically a few to several discrete elements that could have led to the problem occurring.
Then begin with Element 1a and ask why and how that element (1a) could have occurred.
This will give you your second-row elements.
Then move to Element 1b and do the same thing, and so on.
It is not necessary to use a computer to do this;
use Post-It notes to stick on the wall and move them around as needed.
An innovation for the fault tree was creating the linkage between how a fault tree functions and the logic of 5 Whys,
the problem-solving approach that involves asking several iterative Whys or Hows to get to the root causes of a problem.
The fault tree is called the visual analog of the 5 Whys,
because it allows you to drill down into the causal factors to look for root cause.
But, expanding beyond the 5 Whys, this tool allows you to see where bifurcations (or trifurcations, etc.)
occur in causality (i.e., typically there are a couple to several reasons acting in tandem as to why a particular thing went wrong,
so you can capture all of them) [1] .
You no longer have to use these two tools (5 Whys or fault tree) in isolation.
They are two forms of the same inductive reasoning.
Figure 1. FTA diagram with first and second row elements
Sentinel Event details
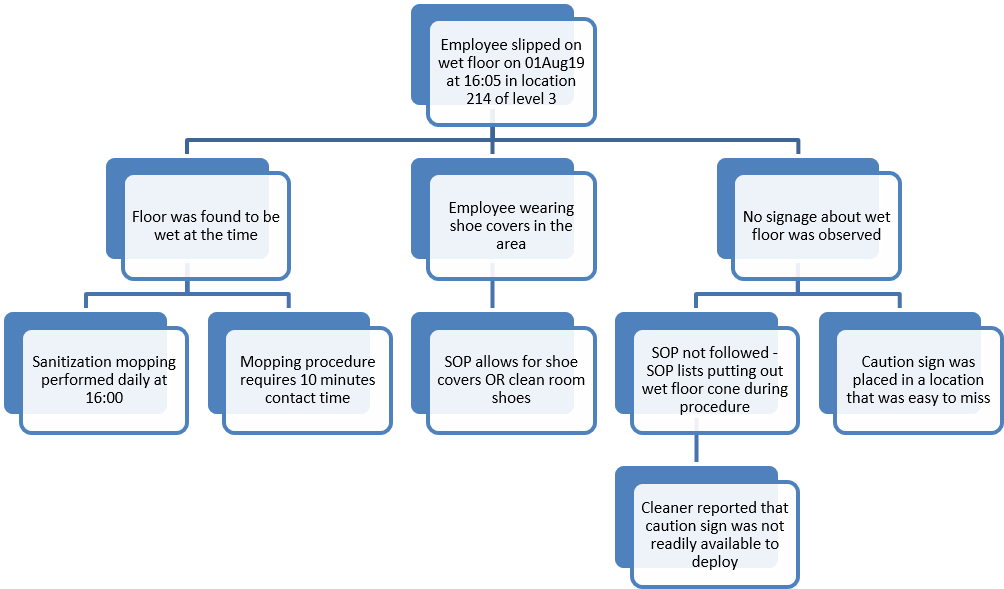
For the sentinel event in figure 2, it is best is to include as much relevant event information as possible: Who, what, when, where, and how are all elements to be included if appropriate. Often, in this situation (and in the head of a fishbone diagram), the problem would be wrongly abbreviated as something overly simplified such as employee slipped on floor. That doesn’t detail the elements that matter to a proper investigation:
where (if there’s a systemic spatial area that keeps causing issues)
what time (in case time is an investigative factor of note)
the nature of the situation (i.e., wet floor)
Figure 2. FTA diagram for nurse fall on wet floor
Row 1: Elements
1a. The floor was found to be wet, and that’s related to the falling event.
1b. The employee was wearing shoe covers at the time of the fall.
1c. There was no sign observed by the employee at the time of the event.
Row 2: Causative Elements (5 Whys)
[2a]. Now let’s go to the second interrogative row, beginning under floor was found to be wet…:
[2a1]. Investigation determined that a sanitization mopping of that area of the facility occurs daily at 16:00, which was in fact about 5 minutes prior to the employee’s fall.
[2a2]. Also answering the question of why the floor was found to be wet, there is a separate branch that the cleaning SOP requires enough water and cleaning fluid to be used such that the floor is wet for a minimum of 10 minutes (for adequate microbial activity).
[2b]. Then moving to the middle element, why was the employee wearing shoe covers?
[2b1].
Because it was allowed per the procedure SOP(either shoe covers OR cleanroom shoes). The shoe covers are an important contributory factor
because the tacky material on their bottoms, which is supposed to help the shoe covers provide a bit of friction
(rather than acting like a sock), actually gets more slippery when wetted,
and so shoe covers should never be allowed in areas where there is a potential for liquids to be present on the floor.
If the event aetiology isn’t systematized in this way, you’re basically tacitly acknowledging that a certain proportion of slips and falls will occur every week, month, or year by giving employees the option to wear shoe covers when you have data to suggest they become slippery and dangerous when they’re wet.
[2c]. And, finally, we get to the right-most elements underneath no signage,
[2c1]. where we find that either the SOP to have the facility cleaner place signage on the floor during the procedure wasn’t followed
[2c2]. OR potentially that the sign was placed but wasn’t seen (or remembered) by the employee.
Row 3: Deeper Level Causative Elements (5 Whys)
[3c]. And, finally, we get to the third level element underneath no signage,
[3c1]. the cleaning personnel couldn’t find the sign to install at point of use during the mopping and 10-minute residence time of wet floor.
The Futility of Signage
Figure 3.
This could be a deviation if the sign wasn’t found and used as specified in the SOP; however, note that whether or not it is a deviation is not the same as whether or not the procedure is effective.
A sign in this case is entirely unhelpful, so it wouldn’t matter if the sign was there or not, but you still could have a process deviation incurred for not following the procedure. To this point, please consider how your SOPs are written and whether they actually prescribe truly effective activities!
People don’t read signs, and if they see them, they may not cognitively register them.
Do not have a preventive retraining on the topic of employees need to read signs. Signs do not systematically cause or prevent behavior.
Establishing Robust CAPA: The Whole Point Of Fault Tree Analysis
[CAPA=Corrective & Preventive Action]
As you probe this fault tree more deeply, you should start by asking why sanitization mopping is performed at 16:00 each day? and why the procedure requires 10 minutes of contact time? In thinking about solving the root cause (employee fell), you could begin to think that, while a daily mopping may be required for facility upkeep and for environmental monitoring purposes, it could be done at a different time when there is reduced foot traffic. This would prevent the human: wet floor interaction and therefore make it much less likely for someone to have a fall hazard. Maybe you could even consider changing cleaning regimens to something that doesn’t require 10 minutes of dwell time. And/or you could disallow shoe covers to be worn if your facility data suggests that clean room shoes are associated with fewer slip/fall events. Let the data be your guide to the best solutions and combine approaches for maximum likelihood of success.
Warning in Root Cause Analysis
creating CAPAs that don’t address the root cause(s) of issues is worse than not doing anything at all. You may cause unintended consequences!